
Many people have Chronic Obstructive Pulmonary Disease, but what is COPD and what can physical therapy do for it?
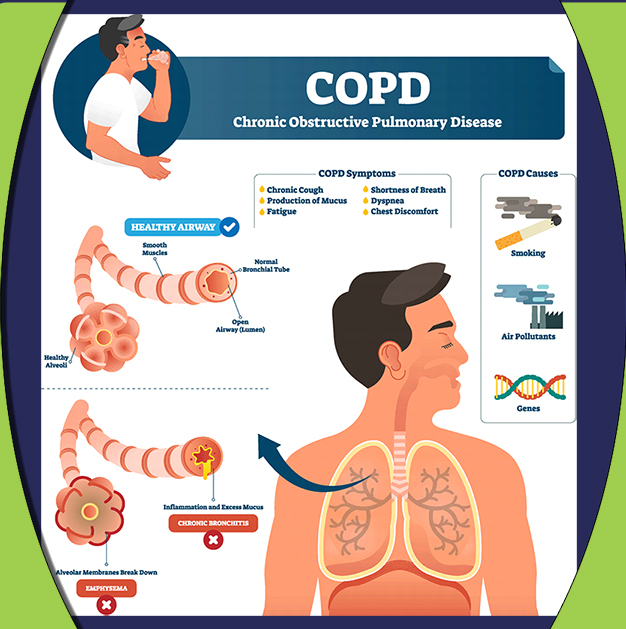
Chronic Obstructive Pulmonary Disease is caused by destruction of the cells in the lungs from chronic inflammation. It can be caused by environmental hazards such as chemicals and smoke, but can also be caused by genetic factors. Due to the inflammation, the lung tissue where air and carbon dioxide is exchanged to breath become enlarged, and air is obstructed. This makes it difficult to breathe, especially when exhaling as air is trapped. Overall most people with COPD have difficulty with expelling carbon dioxide, leaving them short of breath as the lungs cannot completely fill with air, obstructed by carbon dioxide.1,2
Common COPD symptoms include:
- Shortness of breath, especially with physical exertion
- Wheezing
- Chest tightness
- A chronic cough that may produce mucus (sputum) that may be clear, white, yellow or greenish
- Frequent respiratory infections
- Lack of energy
- Unintended weight loss (in later stages)
- Swelling in ankles, feet or legs
- Hypertrophied and shortened accessory inspiratory muscles due to overuse which may cause rounded shoulders, forward head, and/or kyphosis
How is COPD diagnosed?
A patient is diagnosed through a chest x-ray. The extent of the COPD is diagnosed with a pulmonary function test. The testing measures the quality of the patient’s breathing. Based on the symptoms of the patient and the test, a set of guidelines to help clinicians and patients was established, called Gold’s Classification.
Table 1: Classification of severity of airflow limitation in COPD (classification based on post-bronchodilator FEV1 in patients with FEV1/FVC<0.7)
| Guideline | Disease severity | FEV, range |
| GOLD1 | Mild | FEV, ≥80% predicted |
| GOLD2 | Moderate | 50%≤ FEV, <80% predicted |
| GOLD3 | Severe | 30%≤ FEV, <50% predicted |
| GOLD4 | Very severe | FEV, <30% predicted |
How is COPD treated?
There is no cure for COPD. However, physical therapy can help improve overall functional ability for activities of daily living.
Physical therapy techniques for COPD:
- Pulmonary rehabilitation
- Airway clearance techniques
- Breathing exercises/controlled breathing
- Postural education
- Exercise
- Smoking cessation
- Weight control
What does the research say about physical therapy techniques for COPD?3
- There is a growing body of evidence that interval training in patients with chronic obstructive pulmonary disease (COPD) significantly improves exercise tolerance and quality of life.
- Interval training has shown to allow leg exercise to be sustained at a high intensity, which otherwise would not be tolerable. Interval training can be used in patients with advanced COPD, who are unable to sustain exercise intensities sufficiently long enough to obtain exercise benefits because of oxygen limitations. Importantly these patients can endure high-intensity interval training in a rehabilitation setting for long periods of time with lower symptoms of dyspnea (shortness of breath) and leg discomfort compared to the conventionally implemented continuous training.
- Brief bouts of high-intensity interval exercise (HIIT) in COPD do not exacerbate the oxygen requirement.
- Most randomized trials have shown that interval training in the rehabilitation setting is equally effective to continuous training in terms of improving exercise capacity and health-related quality of life in COPD patients with varying disease severity. Both training modes elicit similar training responses in the legs, while interval training induced less symptoms of dyspnea (shortness of breath).
- A few studies have shown contradictory results reporting no differences in symptoms between training modalities. Differences between studies might be attributed to the interval durations.
- “Although a recent systematic review of 8 randomized control trials (388 patients) failed to reveal the efficacy of interval training over that of continuous exercise for enhancing exercise tolerance and quality of life in patients with severe COPD, the authors presented some limitations (training protocols heterogeneity, small sample sizes), suggesting that further research is needed in order to reveal the superiority of interval training in severe COPD. Issues that were not fully addressed in previous studies (such as performing comparisons among training groups exercising at different total work-loads during the course of rehabilitation) need to be clarified by future research.”
- Recommendations from the Research with a Cycle Ergometer or Stationary Bike:
- Frequency: 3-4 times weekly.
- Interval mode: 30 seconds exercise period with 30 seconds rest or even 20 seconds exercise – 40 seconds rest.
- Intensity and duration: initially familiarize the patients on the cycle ergometer at an intensity equivalent to 80% of the maximal work load for 15 to 20 minutes for the first 3 to 4 sessions. The Borg Scale of perceived exertion can be used to more easily monitor exercise intensity. Increase training work load by 5% to10% of peak capacity when patients rate their perceived dyspnea as moderate. If the 10-point Borg scale is used to describe exercise intensity, most exercise should be performed between 5 to 6 intensity for the legs and 3 to 4 for dyspnea.
- Increase total exercise time from 30 to 90 minutes per session (including rest periods), at intensities that progressively reach 150% of the baseline maximum work load.
- Suggest pursed-lip breathing during rest periods to increase tidal volume and reduce breathing frequency.
- Teach patients to perform all daily activities (eg, stair climbing, uphill walking) at an interval mode consisting of short bouts of activity lasting 10 to 15 sec and rest periods of 15 sec.
- Give written instructions to the patients for home practice.
References:
- Hillegass, E. (2017). Essentials of Cardiopulmonary Physical Therapy (4th ed.). St. Louis, MO: Elsevier.
- Goodman, C.C., Fuller, K.S. (2015). Pathology Implications for the Physical Therapist. (4th ed.) St. Louis, Missouri: Elsevier Saunders.
- Kortianou, E. A., Nasis, I. G., Spetsioti, S. T., Daskalakis, A. M., & Vogiatzis, I. (2010). Effectiveness of Interval Exercise Training in Patients with COPD. Cardiopulmonary physical therapy journal, 21(3), 12–19.